Clinical features of vasculitis as a whole (for written):
- fever, fatigue, weight loss, night sweats,
- skin rash, skin ulceration,
- myalgia, arthralgia,
- cough, hemoptysis, epistaxis, diplopia, deafness,
- abdominal pain, oral ulcer,
- tingling, numbness
Class of small vessel vasculitis;
- Primary (ANCA Associated vasculitis
- MPA
- GPA (WG)
- EGPA
- Secondary: Causes: RA, SLE, Cryoglobulinemia, HSP etc
MPA:
- RPGN-more
- Alveolar hemorrhage
- Other- skin, gut, neuropathy, pleural effusion
- Anti MPO positive
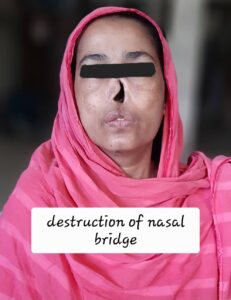
GPA:
- Pulmonary-more involvement
- Epistaxis, nasal crusting, sinusitis
- Loss of nasal bridge /saddle nose
- Hemoptysis, mucosal ulceration
- Migratory pulmonary infiltrate/nodule
- Kidney: RPGN
- Ear: Deafness (inner ear)
- Eye: Proptosis, diplopia, color vision, loss of vision
- Anti-proteinase (PR3) positive




EGPA:
- Eosinophilia- distinguishing feature
- Long H/O: allergic rhinitis, nasal polyposis, late onset asthma(difficult to control)
- Acute typical presentation (Triad)
- Skin lesion- purpura, nodule
- Mononeuritis multiplex (symmetric)
- Eosinophilia
- Pulmonary infiltrates
- Serositis: pleural / pericardial effusion
- Abdominal pain- mesenteric vasculitis
- anti MPO, PR3 ab positive
Investigation (for all):
- WBC: leukocytosis; Eosinophilia→ EGPA
- CRP, ESR- high
- p-ANCA, c-ANCA, anti-MPO, anti-PR3
- Complement- normal/high
- RFT: creatinine with eGFR, urine analysis
- MRI of upper airway, chest, nasal passage : abnormal in GPA
- Biopsy from lesion
- kidney: segmental inflammation, necrosis, crescent formation
- skin, sinus, nasal mucosa
Treatment (for all):
Induction of remission: for organ threatening AAV
- High dose Glucocorticoids plus IST (cyclo/MMF)
- Pulse IV methylprednisolone: 0.5-1.0 gm for 3 days, plus
- Cyclophosphamide: 15 mg/kg, every 2 weeks for 3 months
Fulminant lung disease/RPGN
- Plasmapheresis /Plasma exchange
Maintenance therapy
- LD Glucocorticoids and azathioprine//MMF/MTX
- In case of EGPA: glucocorticoids+ mepolizumab → decrease risk of relapse
Monitoring: Long term monitoring needed→ high chance of relapse
- Urine for blood, protein
- S. creatinine
- FBC, CRP, ESR
- Lung function
- MPO, PR3 antibody titres
Reference: Davidson, Harrison